I feel awful for Taylor Fedun. This player was a guy is 23, an undrafted free agent, and was not supposed to come close to making the Edmonton Oilers starting line-up. This preseason, he was giving management something to really chew on given his strong play.
... then
this happened. The view isn't great but you don't want to a clear view of someone fracturing their femur. Trust me, it's
not pretty. Now, Fedun's entire playing career is in jeopardy not just because he will have to fight hard to make a team again, but also because of how
catastrophic a femur fracture can be and the loooong (but very important) road through rehab. Unfortunately, it's not an unheard of injury. People in the hockey community know what happened to Kurtis Foster almost three years ago and how long it took for him to recover. Those who watch football may remember Vikings' E.J. Henderson's injury in 2009 and his slow but
eventual return.
 |
| Photo source: myhealth.alberta.ca |
 |
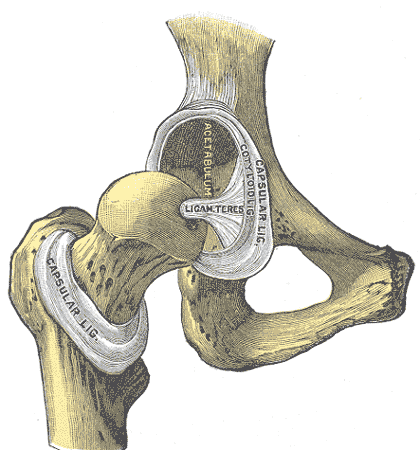
| Picture source: Wikipedia |
The femur is the longest and strongest long bone in the body. It is the only bone that runs through your thigh and forms joints at the hip and the knee. In healthy people, it is very difficult to break and these fractures are usually seen either in high velocity motor vehicle accidents or falls from a height.
Surrounding the femur are three muscle compartments - anterior (to extend the knee and flex the hip), medial (to adduct the hip), and posterior (to flex the knee and extend the hip). The strong pull of all these muscles can actually lead to a greater angle of the fracture and separation of the fragments. Also, it has a very rich blood supply which can be disrupted from the fracture and cause a lot of bleeding. Fortunately, there is often enough supply from the blood vessels in the bone itself that can provide nutrients to help with healing.
Definitive treatment involves orthopaedic surgery where a nail is inserted to help the union of the two fragments and enable strong fixation. It is associated with 98-99% union rate.
The Oilers have already revealed these following details via twitter:
Fractures can be classified (via the Orthopedic Trauma Association) as simple, wedge, or complex. Complex fractures occur when there is no contact between the main fragments, and there is usually (not always) more than two fragments broken off. A fracture is usually classified in many other ways including the angle of the proximal and distal fragments, if the bone broken through the skin (which would require immediate IV antibiotic therapy), etc. These details were not disclosed though, and understandably so because it is not useful public information.
Also, it's good to hear he went through surgery successfully. Early surgery in this case is usually associated with better outcome.
Below are reasons why this injury is concerning:
1.
It can be life-threatening if not addressed promptly. The rich blood supply of the femur means that a fracture can result in a lot of bleeding. You can lose up to 3 L of blood, although the average is closer to 1 L. FYI, we generally have a total of 5 L of blood in our bodies at any given time. Maintaining adequate volume early (via IV fluids) in the injury is a very high priority. The femoral artery (largest artery in the lower body) and the sciatic nerve (largest nerve in the entire body) run nearby, but because they are surrounded by muscles, they are usually protected from injury.
2.
It is a long road through rehabilitation. Early physical therapy is important, like for many orthopaedic injuries. Of course, each case is different, and activity depends largely on how well the fragments are fixated. Actual
healing of the fracture itself takes anywhere from 3-6 months, and then muscle rehabilitation begins. Baseline function and strength can return anywhere from six months (esp in young patients with aggressive physical therapy) to two years (older patients). Athletes usually take a solid year to return to sports.
Fortunately, prognosis is usually excellent. Complication rates are relatively low. These complications include infection (~1%), malunion (healing at the wrong angle) and/or nonunion (no sign of healing at 3 months) of the bone (3-5%) and neurovascular injury.
It's a long road.
I remember thinking when I was younger that I loved touch-icing because of the odd time the offense beat the icing call and generated an exciting scoring change. Now, I agree with the NHLPA and I can see the likelihood for these serious injuries outweigh the potential for 'entertainment'.
Sources: UpToDate